Lower eye bags or lower eyelid bags are often caused by pseudoherniation of orbital fat from under the eye forward into the cheek, where it is visible as a bulge or “bag”. The orbital septum, which contains the fat, can weaken and allow this forward protrusion of the orbital fat past the lower eyelid, creating an eye bag and also commonly a depressed area, or tear trough, immediately below it. While for mild cases undereye filler and hyaluronic acid filler injected into the tear trough can produce an improvement in the appearance of the undereye area by providing additional volume in an area that is deficient in volume, for cases where the lower eyelid fat is more prominent, the fat itself must be addressed to create the optimal cosmetic outcome.
For more information: https://www.donyoomd.com/services-lower-blepharoplasty.php
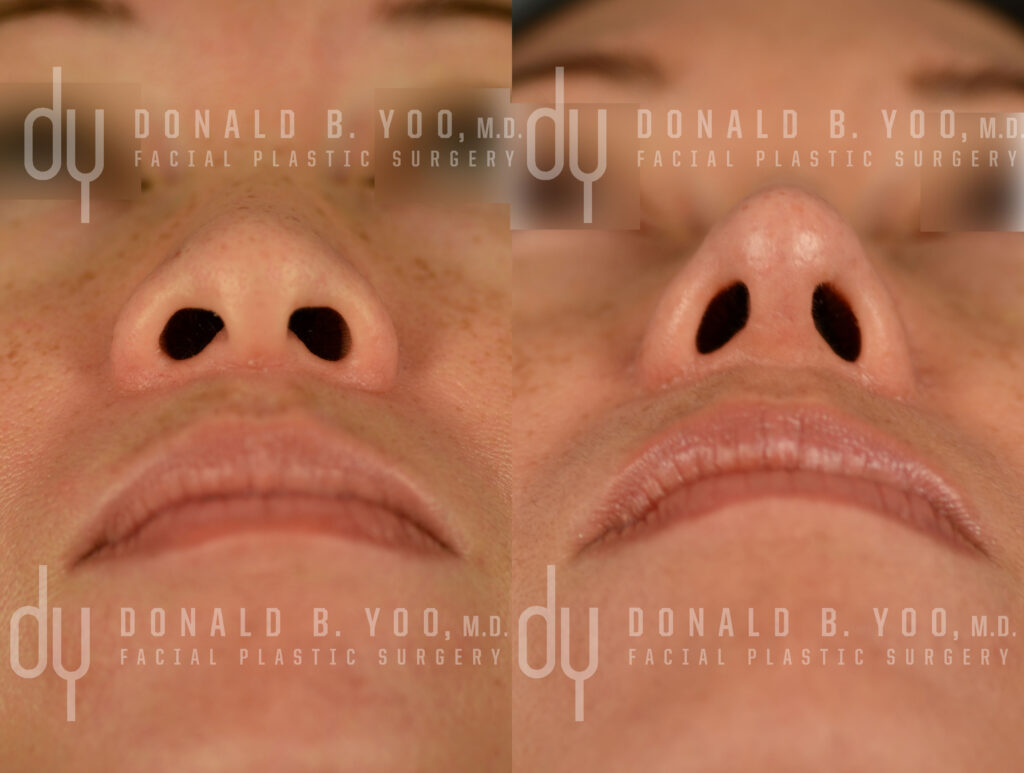
A hidden incision is made within the eyelid, so that no scar is visible. This scarless (transconjunctival) approach allows access to the bulging orbital fat, and it also allows access to the cheeks. After the fat is mobilized the soft tissue overlying the cheek bone is elevated down past the tear trough (orbito-malar groove) to allow for a pocket into which the mobilized fat can be re-positioned. Instead of excising the bulging orbital fat, which with further aging may result in a more aged appearance, the fat is re-positioned into the hollow of the tear trough, acting as a permanent filler to volumize this area. Sutures which remain in place for a week are used to secure the fat precisely in place, during which time the tissue of the cheek will incorporate the newly re-positioned fat. Foam bandages cover the cheeks for a week, and most patients feel comfortable returning to work or school in 2 weeks with their newly rejuvenated appearance.
What is the cause of Eyebags?
Orbital fat that normally cushions the eye, and stays below it, pseudoherniates forward into the cheeks and creates a bulge.
How can I get rid of Eyebags?
Lower blepharoplasty with fat repositioning is a scarless, straightforward way to eliminate the appearance of eyebags without any attendant change in appearance of the eyes.
Does lack of sleep cause eye bags?
Lack of sleep and too much work can definitely contribute to an increased prominence of eye bags. Some people, even with full rest and sleep will still continue to have a prominent appearance of their under eye bags.
Why do I have eye bags at 14?
Some individuals will have genetics and anatomy that predisposes them to having visible under eye bags at a young age. Getting plenty of sleep and rest can help reduce the appearance, but may not eliminate it completely if you are anatomically and genetically predisposed.