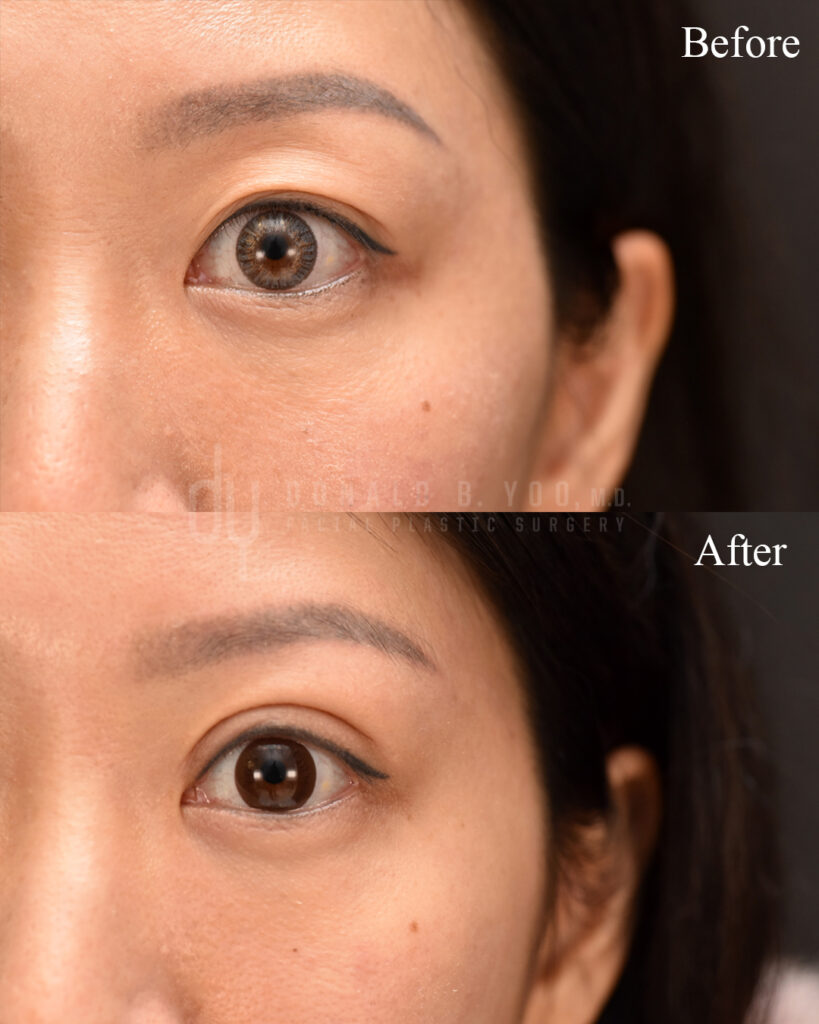
Lower blepharoplasty is one of the most requested procedures for patients bothered by under-eye bags, hollowing, or a tired appearance that doesn’t match how they feel. But not all lower blepharoplasty is performed the same way. The surgical approach — where the incision is placed and how the underlying tissue is accessed — has a major impact on recovery, scarring, and the risk of complications like eyelid retraction.
The two primary approaches are transconjunctival and subciliary. Understanding the difference helps explain why the same procedure name can produce very different results in different hands.
What Is Lower Blepharoplasty Addressing?
As we age, the fat pads beneath the lower eyelid can prolapse forward, creating the appearance of puffiness or bags, while the surrounding tissue can lose volume and support, creating hollowing or a tear trough deformity. Lower blepharoplasty addresses this by accessing and repositioning or removing that fat, and in some cases addressing excess skin as well.
The technique used to access that fat is where transconjunctival and subciliary approaches diverge.

The Transconjunctival Approach
The transconjunctival approach places the incision on the inside of the lower eyelid, through the conjunctiva, with no incision on the visible skin at all. Through this internal incision, fat can be removed or repositioned to smooth the transition between the lower lid and cheek.
Advantages:
- No visible external scar, since the incision is entirely internal
- Lower risk of ectropion or lower eyelid retraction (a pulled-down, rounded appearance to the lower lid), because the orbicularis muscle and lower eyelid support structures are left undisturbed
- Generally faster external recovery, with less visible bruising
Limitations:
- Best suited for patients whose primary concern is fat bulging, without significant excess skin
- Cannot directly address excess or crepey skin, since there is no external incision through which skin can be trimmed
- Requires meticulous technique to reposition fat effectively without an external view of the skin surface
The Subciliary Approach
The subciliary approach places the incision just below the lash line, on the visible skin. This allows direct access to both the fat pads and any excess skin, making it possible to address both prolapsed fat and skin laxity in the same procedure.
Advantages:
- Allows for skin excision in addition to fat repositioning, useful for patients with meaningful skin laxity
- Provides more direct visualization and control over fat repositioning at the skin surface
Limitations:
- Leaves a fine external incision line, though when placed carefully just below the lash line it typically heals to be very difficult to see
- Higher risk of lower eyelid malposition or retraction if the orbicularis muscle and lower eyelid support are not carefully preserved and, when appropriate, reinforced with a canthal support procedure
- Generally a longer recovery window for external swelling and bruising to resolve
Why This Distinction Matters So Much
The subciliary approach has a well-documented association with a higher rate of lower eyelid retraction compared to the transconjunctival approach, largely because it involves more direct disruption of the muscle and support structures of the lower eyelid. This doesn’t mean the subciliary approach should be avoided — for patients with genuine excess skin, it may be the only approach that fully addresses their concern — but it does mean the decision of which approach to use should be based on individual anatomy, not surgeon default.
In my own published research on this topic, comparing the plane of fat transposition in transconjunctival lower blepharoplasty, technique-level decisions like this measurably affect outcomes — reinforcing why a one-size-fits-all approach to lower eyelid surgery doesn’t serve patients well.
Combining Approaches
Many patients are best served by a combined approach: transconjunctival fat repositioning to address bulging and volume loss, paired with a very conservative skin pinch or resurfacing to address minor skin laxity — without a full subciliary incision. This combined strategy is often able to achieve the benefits of both approaches while minimizing the risks associated with a larger external incision.
Recovery Comparison
| Transconjunctival | Subciliary | |
|---|---|---|
| Visible scar | None | Fine line below lash line |
| Best for | Fat bulging, minimal excess skin | Fat bulging with excess skin |
| Retraction risk | Lower | Higher if not carefully performed |
| Typical bruising/swelling | Resolves faster | Longer resolution window |
| Can address skin laxity | No | Yes |
Frequently Asked Questions
Which approach is better?
Neither approach is universally “better” — they address different problems. Transconjunctival is generally preferred when the primary concern is fat bulging without excess skin, since it avoids any visible scarring and carries a lower risk of eyelid malposition. Subciliary becomes necessary when there is meaningful excess skin that also needs to be addressed. The right choice depends on your specific anatomy.
Can under-eye bags be treated without surgery?
Mild fullness or early hollowing can sometimes be improved with fillers to soften the transition between the lower lid and cheek. However, fillers cannot remove or reposition prolapsed fat, and in patients with significant bulging, filler can sometimes make the appearance of bags more noticeable rather than less. A consultation can help determine whether your concern is better suited to filler or surgical correction.
What is lower eyelid retraction, and how is it avoided?
Lower eyelid retraction occurs when the lower lid is pulled downward, creating a rounded or “scleral show” appearance where more white of the eye is visible beneath the iris than normal. It is more commonly associated with the subciliary approach, particularly when the orbicularis muscle and lateral canthal support are not carefully preserved or reinforced. Meticulous technique and, when indicated, an additional canthal support procedure significantly reduce this risk.
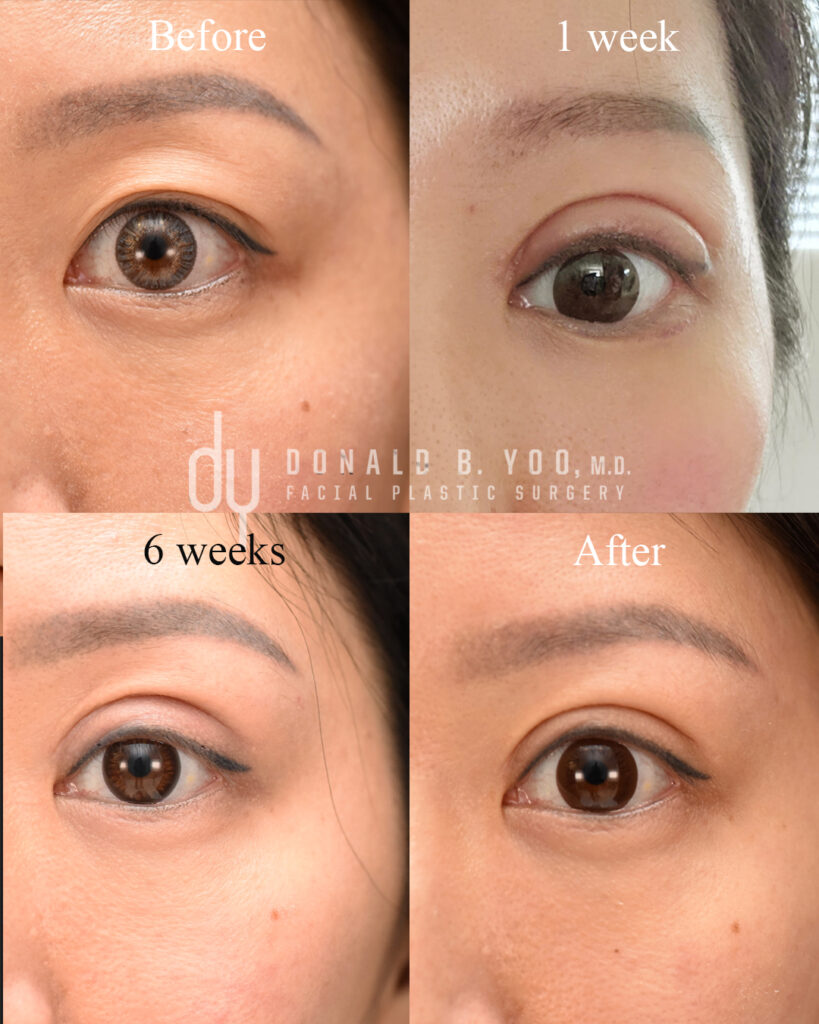
How long is recovery after lower blepharoplasty?
Initial swelling and bruising typically improve significantly within the first one to two weeks, with subtler swelling continuing to resolve over the following month. Recovery tends to be faster after a transconjunctival approach than a subciliary approach, given the difference in how much external tissue is disrupted.
Will insurance cover lower blepharoplasty?
Lower blepharoplasty performed for purely cosmetic reasons, addressing under-eye bags or hollowing, is not typically covered by insurance. This differs from certain upper eyelid procedures, which may be covered when performed to correct a functional vision obstruction.
Final Thoughts
The approach used for your lower blepharoplasty should be determined by your individual anatomy and goals, not by which technique a surgeon defaults to for every patient. During consultation, I evaluate skin quality, fat distribution, and lower eyelid support to recommend the approach — transconjunctival, subciliary, or a combined strategy — most likely to give you a natural, well-supported result.
If you’re considering lower eyelid surgery and want to understand which approach fits your anatomy, I encourage you to schedule a consultation.
Donald B. Yoo, M.D., F.A.C.S. is a double board-certified facial plastic surgeon and Medical Director of HALO Beverly Hills, specializing in revision and Asian rhinoplasty, alarplasty, lower blepharopalsty, and Asian blepharoplasty. His office is located at 433 N. Camden Drive, Suite 970, Beverly Hills, CA 90210.